TSICU:Main
This is the main page for Harbor-UCLA Trauma SICU
Admin Updates & Reminders
Media:SICU Intern Guide.pdf
General Administrative
- TSICU Structure & Function
- Monthly Call Schedule
- Trauma/SICU Attending
- SICU Fellows media:July 2019_Fellow.pdf
TSICU: Weekly Schedule
Educational Conferences
TSICU:Clinical Documentation
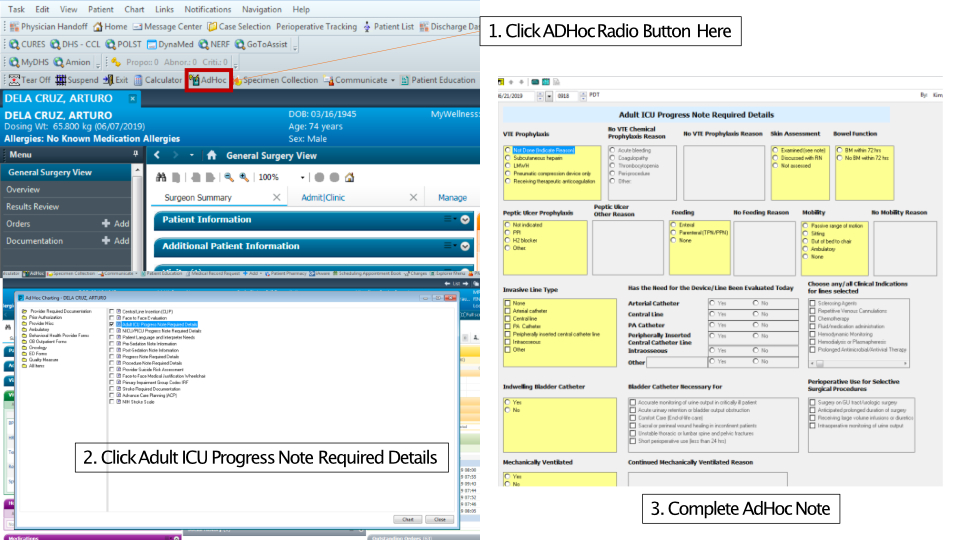
- Adult ICU Progress Note Required Details. Media:Ad Hoc.jpg
- This AdHoc Note is to be completed every day and PRIOR to starting the daily ICU Progress Note
{kind=link}
- Core Measures/Common Conditions
- Hospital Acquired Pressure Injuries (HAPIs)
- Pressure injuries are to be documented in the medical record (size, stage)
- Consult wound care team for orders regarding wound care management
- FAST HUGS BID
- Ensure that his is completed for every TSICU patient daily
- Code Status
- Clarify code status with patient or patient's next-of-kin, DPoA or SDM, as soon as feasible
- Ensure this is clarified on the medical record
- Advanced Directives
- Medication Reconciliation
- Performance Improvement and Patient Safety
- Safety Intelligence (SI)
SICU Order Sets
Mandatory Call Criteria
Consult Services
Rapid Response Team (RRT)
- Members of the on-call trauma surgery team, including the Trauma Attending, respond to all Surgical Rapid Response pages/overhead calls
- Harbor:Codes
Disaster & Surge Plan
Contact Information
Patient Care Management
General
- Housestaff Expectations
- Roles and Responsibilities
- Communication & TeamSTEPPs
- Conduct of Morning Rounds
- Handoffs
Admission to the TSICU
*Every admission to the TSICU requires Trauma/SICU Attending approval
From the Emergency Room
- Following approval by the Trauma/SICU Attending, the charge or relief RN will be notified and a unit bed assigned
- At minimum, the following patient information should be conveyed (Name, MRN, admission diagnosis, clinical condition)
- Bed assignment requires notification of bed control
- An ER RN to SICU RN handoff must take place PRIOR to the patient's arrival in the TSICU
- A formal handoff is to take place between a member of the on-call surgery team and a member of the TSICU team
- iPASS Handoff Tool
- Any clinical concerns or signs of deterioration requires IMMEDIATE notification of the Trauma or TSICU Attending
- TSICU Mandatory Call Criteria
From the OR
- Patients previously admitted to the TSICU
- New TSICU admissions or patients not previously admitted to the TSICU
- OR to SICU Handoff
- Elective operations in which TSICU admission is anticipated should be communicated with the TSICU at least 1 day prior to the elective case
From Monitored or Unmonitored Bed
Interfacility Transfers
Transfers & Downgrades
- Trauma/SICU Attending approval is required for all transfers and downgrades
- Out of network patients will require a minimum of 24 hours of observation in a non-ICU monitored bed PRIOR to transfer
Trauma/ACS Service Patients
Non-Trauma/ACS Service Patients
Tests & Orders
Labs
Point of Care
- POC devices immediately available in the TSICU include:
- iSTAT
- Note on cartridges
- Hemacue
- Glucometer
- iSTAT
- Thromboelastography (TEG)
Diagnostic Imaging
- CXR
- Orders for non-urgent CXRs are to be placed at the time of morning rounds PRIOR to the desired day (i.e. Tuesday am CXRs should be inputted during Monday am rounds)
- Per our agreement with the Radiology Department, CXRs in the TSICU are schedule for 07:00am q day
- Ultrasound
- CT scan
- MRI
Bedside Echocardiogram
EEG (including Ceribell)
Antibiotics
Equipment & Supplies
- TSICU Map media:TSICU Layout.pptx
- Any broken or defective equipment should be reported IMMEDIATELY to the charge RN, nurse manager, or Dr. Kim
- Surgery house staff are responsible for cleaning up after all procedures. This includes, but is not limited to:
- Disposing of all sharps in the appropriate sharps container
- Cleaning all used or dirty equipment with the appropriately supplied cleansing wipes or agents
- Returning all used equipment to their assigned parking spots in the TSICU or B-bay
- Line Carts
- Ultrasound Machines
- B-bay Supplies
Procedures
- Informed Consent
- iMed Consent
- Blood Transfusion
- ICU interventions
Occupational Exposure
Referral to One Legacy
Death Packet Checklist
Core Clinical Conditions & Management
Shock
- Undifferentiated shock
- Hypovolemic
- Cardiogenic
- Distributive
- Resuscitation Endpoints
- Ultrasound: In Shock and Hypotension
Assessment of Fluid Responsiveness in the ICU
Pulmonary
Initiating Mechanical ventilation (main)
- Ventilation Settings
- Ventilation modes
- Recruitment maneuver
- Ventilator associated lung injury
- Ventilator high pressures
Discontinuing Mechanical Ventilation
- TSICU Extubation Standard Operating Procedure
- Ventilation weaning
- Extubation
Noninvasive ventilation
Acute Respiratory Distress Syndrome
Advanced Modes of Ventilation
Renal
Acute kidney injury
Acid-base disorders
Electrolyte abnormalities
Rhabdomyolysis
Uremia
Renal Replacement Therapy
- CVVHD
- IHD
Sepsis & Septic Shock
Infections in the ICU and Appropriate Selection of Antibiotics
Post-operative fever
Ventilator Associated Event (VAE) formerly known as Ventilator associated pneumonia (VAP)
Catheter Associated Urinary Tract Infection
Central Line Associated Bloodstream Infection
Surgical Site Infections
- Superficial
- Deep
- Organ Space
C- difficile Infection
Harbor:Infectious Disease Threats
Cardiovascular
Arrhythmias
Hypertensive Emergency
Nontraumatic thoracic aortic dissection
Acute limb ischemia
Hepatic & GI
Liver Failure
Abdominal compartment syndrome
Nutrition Therapy including Stress Ulcer Prophylaxis
Refeeding syndrome
Disseminated Intravascular Coagulopathy
Traumatic Brain injury
Mild traumatic brain injury
Moderate-to-severe traumatic brain injury
Spinal Cord Injury
- ASIA Score
- Spinal cord syndromes
Neurologic Emergencies
Altered mental status
Seizure
Alcohol withdrawal seizures
- CIWA Protocol
CVA
Management of Hemorrhage in Patients on Antithrombotic Therapy
Pain, Agitation, Delirium, Immobility, and Sleep (PADIS)
RASS
Delirium
- CAM-ICU
Endocrine Emergencies
Diabetic ketoacidosis
Nonketotic hyperglycemia
Hyperosmolar hyperglycemic state
Hypoglycemia=
Diabetes medications
Adrenal crisis
Pheochromocytoma
Thyroid storm
Myxedema coma
Hypothyroidism
Diabetes insipidus
Venous Thromboembolism
- DVT
- PE
Educational Resources
- Numbered list item
Goals & Objectives - MS4
Goals & Objectives - PGY-1/PGY-2
Goals & Objectives - Fellow
Online Resources
Recommended Readings
Procedures
Airway & Breathing
Intubation
- TSICU Intubation Protocol
Surgical Cricothyroidotomy
Bedside Percutaneous Tracheostomy
Fiberoptic Bronchoscopy
Chest tube insertion
Pigtail catheter thoracostomy
- Step-by-step instructions
- Procedure on a real patient
- Can be considered for spontaneous or small traumatic pneumothorax
Thoracentesis
Invasive Hemodynamic Monitoring & Access
Central Venous Catheterization
- Internal jugular central venous catheter (CVC) insertion
- Subclavian central venous catheter (CVC) insertion
- Femoral central venous catheter (CVC) insertion